Why We Must Change?
Paul Ehrlich (Germany; 1854–1915), the founder of chemotherapy, postulated more than 100 years ago that chemicals, just as histologic dyes, have selectivity for certain components in cells and tissues, and, therefore, could be used to fight against specific human diseases if the culprit was identified and targeted.
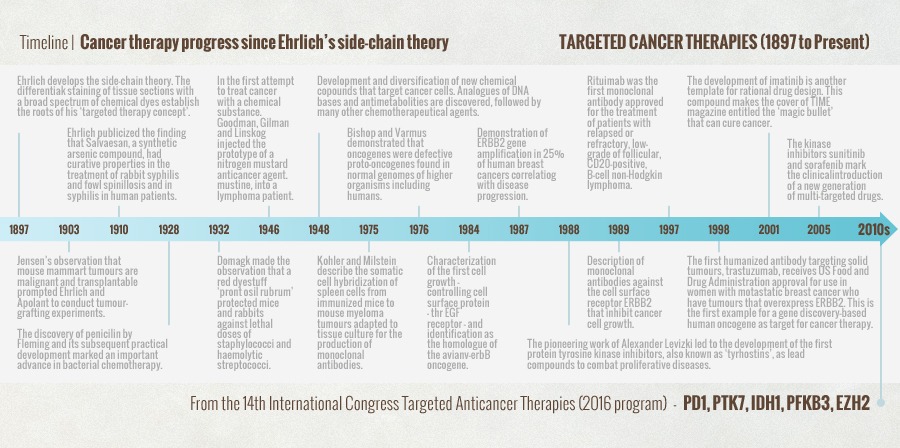
This concept has inspired generations of cancer researchers to pursue drugs and biological products that selectively target cancer cells or molecular events that are believed to drive the malignant phenotype, while doing little damage to normal cells. The following chart summarizes almost 120 years of progress in targeted cancer therapy.
PARADOXES OF OUR CANCER THERAPEUTIC PROGRESS
During the last 30 years, advances in molecular biology and cancer genetics have expedited cancer drug development and targeted therapies tremendously. Paradoxically, at the same time, cancer is threatening human society more than ever before in recorded medical history. As of 2014, cancer became the most common cause of death worldwide [1]. In the United States, cancer is the leading cause of death due to disease for children and adolescents between the ages of 4 and 14 [2], and for all adults except for the elderly [3]. In the U.S. alone, approximately 1,600 men, women, and children die every single day from cancer [4]. About 20,000 people die daily from cancer in the world [1]. Some journalists have compared this to approximately 100 plane crashes per day without survivors.
To better appreciate the magnitude of the problem, in 2010, an estimated 8 million cancer deaths occurred worldwide. By 2030, this estimate is expected to increase to 17 million cancer deaths per year [1]. Although many factors play a role in these figures (pollution, aging populations, etc.), none is more important than the fact that with our current medical treatments involving chemicals, biologicals, and radiation, all common cancers affecting humans (breast, lung, colon, stomach, pancreas, ovarian cancers, melanomas, etc.) remain as incurable and lethal today as they were 100 or 200 years ago, if they advance beyond curability with surgery (and become inoperable or metastatic). Today, only approximately 2% of all cancers can be cured with drugs, biologicals, and radiation (such as some rare leukemias, lymphomas, and germ-cell cancers) [5-7].
THE FALSE POSITIVES OF ONCOLOGIC PROGRESS
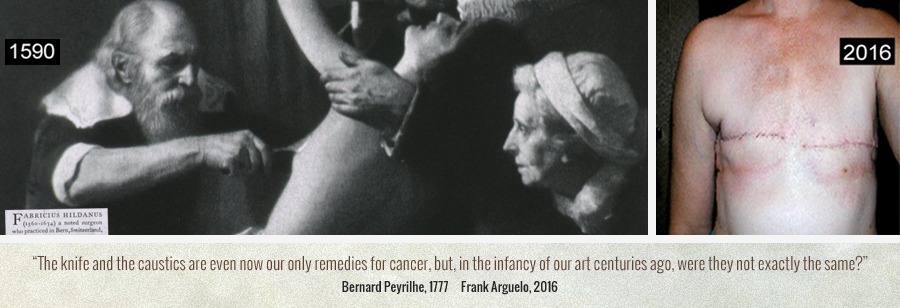
The distrust in our ingenious pharmacological and biological therapies for cancer is evidenced by the fact that we continue removing precious and meaningful organs from women as soon as a cancer the size of a lentil or a pea is discovered in their breasts. In other words, despite our apparent exceptional progress in molecular and genetic therapeutics of cancer, we continue removing one or both breasts and emptying the axillary pits from lymph nodes in women as young as 25, in the same way we have been doing for the last 500 years (see image below). What hopes can we offer to a patient with locally advanced or metastatic breast cancer?
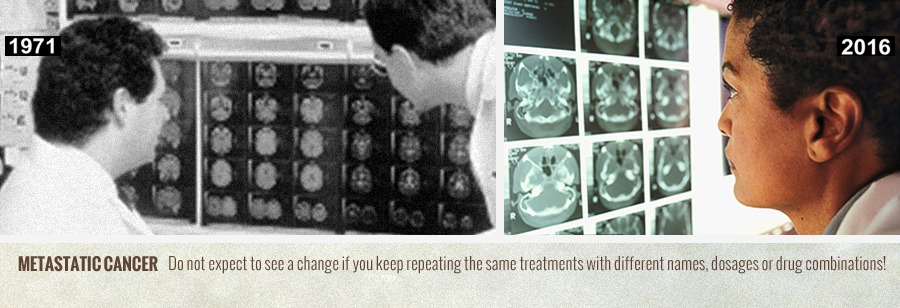
On the other hand, the two main reasons for patients with metastatic cancer to undergo chemotherapy are to live longer and to live better. A recent study involving 312 patients with metastatic disease has found that such treatment achieves neither of those goals. Researchers examined the effect of chemotherapy on patient quality of life in the last week of life as a function of patients’ performance status, which ranks their ability to perform activities such as be ambulatory, do work and handle self-care. They found that those patients have a significantly worse quality of life during their final weeks than those patients who did not receive chemotherapy, according to the study published in JAMA Oncology in September 2015. In addition, the highest functioning patients entering the trial resulted in those whose quality of life in the last week of life was “significantly and meaningfully lower than in those not receiving chemotherapy” [8].
REFERENCES
- Stewart BW, Wild C, editors. World cancer report 2014. Lyon, France: International Agency for Research on Cancer, World Health
Organization; 2014. - Ward E, DeSantis C, Robbins A, Kohler B, Jemal A. Childhood and adolescent cancer statistics, 2014. CA Cancer J Clin. 2014;
64:83-103. - Twombly R. Cancer surpasses heart disease as leading cause of death for all but the very elderly. J Natl Cancer Inst. 2005;
97:330-331. - American Cancer Society. Cancer facts & figures 2014. Atlanta: American Cancer Society; 2014.
- Bailar JC, 3rd, Gornik HL. Cancer undefeated. N Eng J Med. 1997; 336:1569-74.
- Morgan G, Ward R, Barton M. The contribution of cytotoxic chemotherapy to 5-year survival in adult malignancies. Clin Oncol
2004; 16:549-60. - Faguet GB. The Conquest of Cancer: A distant goal. Dordrecht, The Netherlands Springer; 2015.
- Prigerson, HG., et al. Chemotherapy Use, Performance Status, and Quality of Life at the End of Life. JAMA Oncol. 2015;1:778-784.